The foundational pieces of a case is examined in retrospect allow a much-needed review of what is working, what the outcomes for children are, and what the best practices for CPS system professionals are. We take the time to lift up and do a 360-degree review to learn and re-frame the case with a public health lens. How could we have been more effective?
Without bias, and with the child at the center of the reflection, we examine a local case to understand how each of the sectors responded, what the policy implications are, and what the prevention opportunities were. Ultimately, we honestly look at opportunities for improvement so we can move forward more effectively.
The ISPCAN Huddle model is designed as a case-based, multidisciplinary learning and systems improvement approach that examines real child maltreatment cases through a 360-degree retrospective review framed by a public health perspective. The Huddle, created by a panel of global experts in public health, and all related disciplines with Haruv Institute and co-sponsored by the Kempe Center, was designed to train multidisciplinary child protection professionals to strengthen assessment and intervention practices in cases of child maltreatment.
The ISPCAN Huddle is conceived of as a multidisciplinary, global case-based training and learning initiative designed to strengthen child protection systems. The approach involves bringing together professionals across sectors to examine real-world cases of child maltreatment. The Huddle positions child abuse and neglect prevention and intervention as a multi-sector public health issue, requiring coordinated responses from medical, mental health, social work, legal, justice, education, and public health systems. By learning collectively from complex cases, participants work to improve multi-disciplinary team processes, improve communication, avoid repeating mistakes, address gaps in care, and build sustainable improvements within and across countries.
Goals of the ISPCAN Huddle
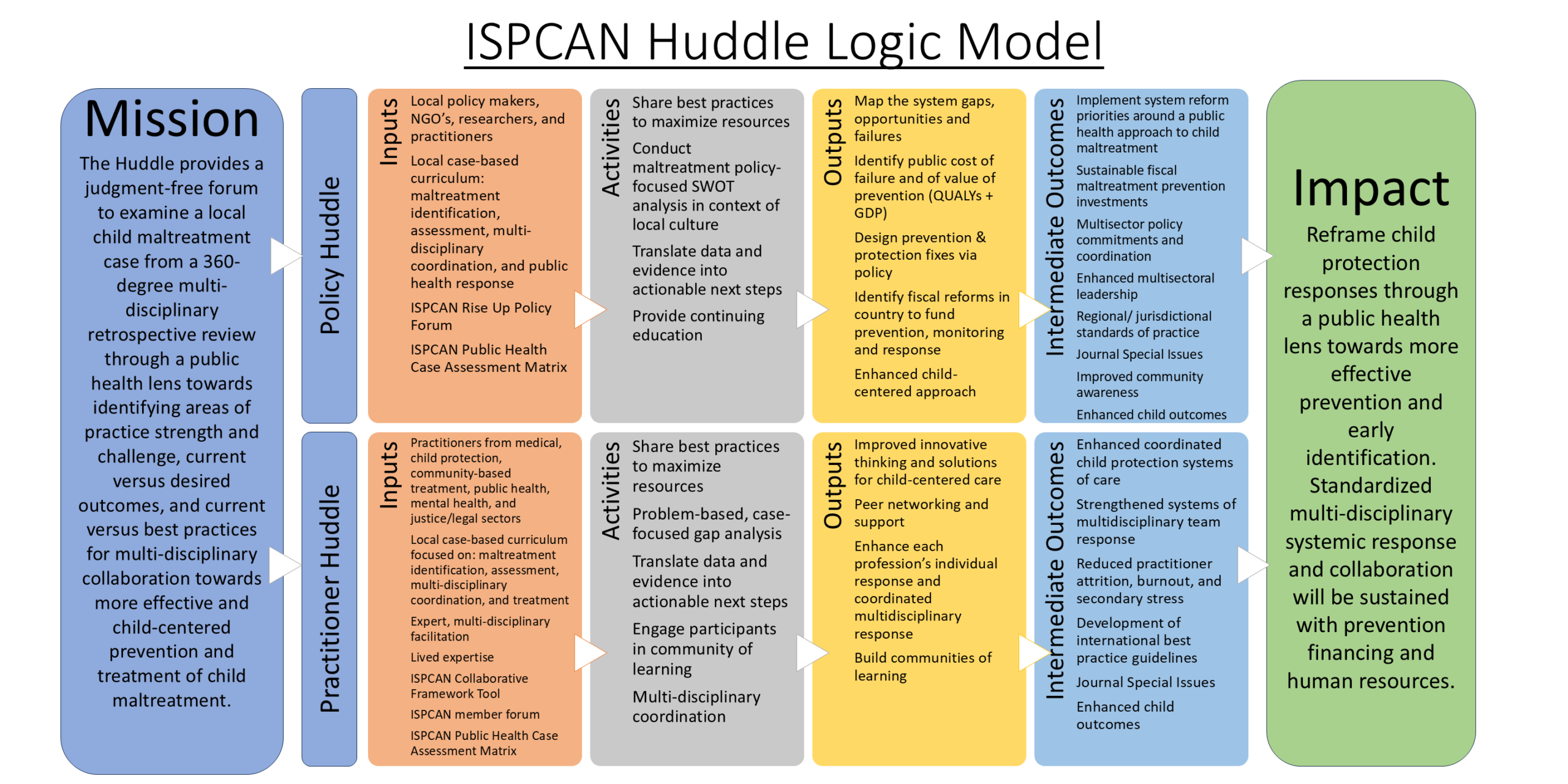
The overall goal of the approach is to translate case insights into actionable strategies that strengthen multidisciplinary coordination and promote more effective, child-centered prevention and response systems. To reach different components of the child protection ecosystem, ISPCAN plans to organize two complementary types of Huddle events that use this case-based methodology but are designed for different audiences. A fundamental assumption is that the events will always be planned to consider the status and current capabilities of the contexts where the events are to be held.
Practitioner Huddles focus on frontline professionals from sectors such as medicine, child protection, mental health, public health, community services, and the legal system. Through facilitated case analysis, these sessions emphasize practical problem-solving, peer learning, and multidisciplinary coordination. The intended outputs include improved professional responses, stronger cross-sector collaboration, reduced practitioner burnout through peer support, and the development of communities of practice that strengthen coordinated systems of care for children. Currently a Practitioner Huddle is being planned in Mexico.
Policy Huddles, in contrast, engage policymakers, NGO leaders, researchers, and system administrators. Using the same case-based analytical framework, these sessions focus on identifying systemic gaps, fiscal implications, and policy reform opportunities. The discussions translate case evidence into policy priorities, prevention investments, and multisector governance strategies that support a public health approach to child maltreatment. The Policy Huddle is being planned for this year in Uganda.
Although the audiences and pathways differ, both types of Huddles are designed to achieve the same broad outcome as depicted in the diagram.
Public health interventions begin with prevention-focused actions that are taken at a whole-of-population level, often through already existing universal service delivery platforms where contact with families occurs (i.e. health, education and child care services), complemented by community-based actions and population-wide strategies. The latter includes information about child safety, awareness raising actions, regulations and controls, and provision of training, resources and supports – for professionals working with families, as well as direct provision of parenting skills and other supports for families themselves.
Child sexual abuse, in the context of culture, family and systems of care will be explored in the African Regional Huddle. How the medical, mental health, and justice systems interacted to protect and heal the child will be examined for an audience of policy makers, so that one child’s story will reframe how we understand the critical need for collaboration of sectors.
Child sexual abuse (CSA) is a worldwide threat to children’s health. Without support, children who experience sexual abuse can have physical, mental, and behavioral problems. All children have the right to life without sexual abuse. When children have experienced sexual abuse, however, they have the right to get the best possible support.
The community’s response to a CSA case is complex because many trained people (professionals) from different fields are needed to properly support the child. This means that multi-disciplinary support teams must be set up to make sure that trained people in the community can respond to the children’s needs. These support teams can then work together to maximize resources, reduce burnout, and better support the victims.